MALLET FINGER INJURIES:
CONSERVATIVE TREATMENT AND PIN CARE STRATEGIES

WHAT IS A MALLET FINGER?
A mallet finger, or terminal tendon rupture, is an injury of the tip of the finger which causes the DIP (distal intrerphalangeal) joint to droop into flexion. This injury is commonly caused by striking the tip of the finger causing a bend further than intended or from advanced stages of arthritis with nodules that eventually fray the extensor tendon. This injury causes a person to be unable to lift the tip of the finger actively.
WHAT ARE SOME OF MY OPTIONS FOR CONSERVATIVE TREATMENT?
For conservative management, therapy is very helpful. It is recommended that the patient be placed in a splint for 6 weeks full time with the DIP joint in at least neutral position. More favorably, it is recommended that the DIP be placed in 10 degrees of hyper-extension. This is required to be worn for 6 weeks WITHOUT a break. Over the counter orthoses, such as a stack splint, are not recommended as they are not a fit for most patients to hold the digit into hyper-extension. The custom splinting is the best option for these patients. Custom splints also allow the patient to move the middle joint, or proximal interphalangeal freely and preserve mobility and function there.

3 Different Options for Orthosis Patterns for Mallet Conservative Management
HOW DO I TAKE CARE OF THE PIN(S)?
Pin care is a very important part of the surgical management of this injury. For surgical management, 1-2, and sometimes 3, pins will be driven through the fingertip to hold the DIP joint into neutral extension. This will be in place 6-8 weeks. Caring for these pins is critical to managing infection and ensuring the success of the mallet procedure pre and post operatively. Pin care is recommended as follows: Q tip dipped in half hydrogen peroxide and half saline solution. The Q tip needs to be dabbed on the pin and around the pin followed by gauze padding off any of the solution that bubbled up. Only using 1 Q tip per pin is required to avoid cross-contaminated. This procedure is to be performed one time per day.

4 Pins Post Operative Mallet Injury
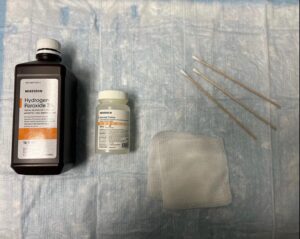
Tools Needed for Successful Pin Care and Cleaning
WHY DO I NEED THERAPY AFTER THE 6 OR 8 WEEKS OF IMMOBILIZATION?
After the immobilization phase, it is time to get the finger moving again! Any exercises that allow activation of the extensor digitorum communis, central slip, flexor digitorum superficialis, and flexor digitorum profundus. Gliding, blocking, and eventually strengthening these structures are critical post operative and post mallet conservative treatment strategies.

 DIP and PIP Blocking Exercises with Use of Donut
DIP and PIP Blocking Exercises with Use of Donut
We are ready and exited to help you at Desert Hand and Physical Therapy with all types of pain and impairments in the hand. If you have a mallet injury or are not sure what is happening with your finger(s), please give us a call at 855-828-6361 and we are ready and excited to help! Click HERE for a link to schedule a new patient appointment!
 If you would like to learn more about Brittany Moya MS, OTR/L, CHT,
If you would like to learn more about Brittany Moya MS, OTR/L, CHT,
please click HERE for her bio